P
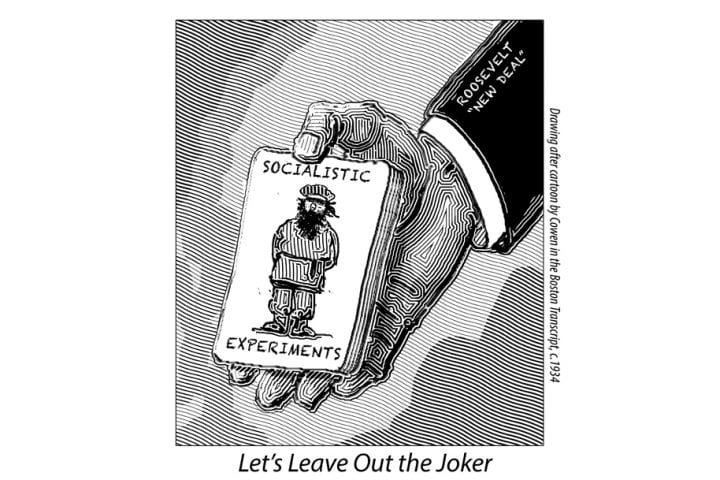
ogressives are nothing if not devotees of history, in whose inexorable benevolence they reveal faith not seen since the days of Peter and Paul. For reasons that are never explained, however, History sometimes misses its entry cues. When it does, progressives are ever ready to provide a nudge or even a hearty shove.
A case in point concerns California’s enactment last October of legislation authorizing physician-assisted suicide—one of those ideas, as progressives so often say, whose time has come. The measure had been introduced earlier in the year, buoyed by the well-publicized death of Brittany Maynard, the fatally afflicted California woman who had moved to Oregon to avail herself of that state’s assisted suicide law. Opposed by members of both parties, the bill effectively died a natural death in the Assembly Health Committee.
Undeterred, the bill’s sponsors decided to shove History onto the stage of a special session of the legislature, where (to make a long story short) the leadership rigged the rules. The measure was rushed through the Assembly, rubber-stamped by the Senate, and presented to the governor.
Governor Jerry Brown, who has rarely found it necessary to disagree with Hisory’s mandates, indicated that he wanted to think deeply before committing himself. After wrestling with his conscience, he pinned it to the mat and signed the bill, making California the fourth state to legalize physician-assisted suicide.
Shoved or unshoved, History has certainly endowed proponents of assisted suicide with generous funding and almost Pavlovian media approval. At the present hour, measures essentially identical to California’s are pending in 14 states, with more states in the wings. Conservative philosophical and religious sentiment that not so long ago had substantial purchase in public opinion is notably weaker now, especially among millennials, who are easy prey for emotional appeals voiced in the language of autonomy and compassion.
The most effective political opponents of assisted suicide these days are organizations like the aptly named Not Dead Yet, a tough-minded defender of the rights of handicapped persons. They argue, correctly, that those who are mentally and physically handicapped will be particularly vulnerable if medically assisted suicide becomes widespread. Once doctors are authorized dispensers of death, considerations of medical convenience or social utility will enter into the doctor-patient relationship in ways unlikely to benefit patients.
Precedent for this may be found in Weimar Germany, where human beings deemed “unworthy of life” because of physical or mental disability were legally euthanized in substantial numbers by willing doctors. Those who say such a thing could never happen here might do well to consider data in our own time from Belgium and the Netherlands. In both countries, the categories of eligible death-seekers have expanded well beyond the terminally ill, and the line between assisted suicide and euthanasia has been substantially erased.
* * *
We have no comparable data from the U.S. as yet, in part because the record-keeping requirements of laws like California’s newly enacted measure are notoriously lax. In the fullness of time, however, we have every reason to believe that we will eventually imitate the Dutch and Belgian examples. Although laws like California’s limit physician-assisted suicide to the terminally ill, courts will almost certainly qualify that limitation on due process or equal protection grounds: if there is a right to determine the time and place of one’s death, how can it be justly confined to the terminally ill? Similarly, if such a right exists, how can it be denied to those who, like comatose patients, are incapable of exercising it?
Constitutional law is already poised to take precisely these steps. Indeed, the Supreme Court came perilously close to declaring a constitutional right to assisted suicide in 1997. Given the current Court’s subsequent embrace of arguments based on autonomous individualism in the gay marriage cases, it may be only a short time before the 1997 precedent gets reversed.
Even in the absence of judicial boldness, medically sanctioned killing may creep in on little cat feet. Shortly after Oregon legalized physician-assisted suicide in 1994, the Oregon Health Plan (a state scheme analogous to Obamacare) announced that it would no longer cover the cost of protease inhibitors, an expensive but effective class of medicines particularly useful in the treatment of HIV/AIDS. Gay activists protested vigorously, and the restriction was eventually lifted.
But consider the disposition of the bureaucrats who proposed the restriction in the first place and what it bodes for our future under Obamacare. That law created a bureaucratic monstrosity called IPAB (Independent Payment Advisory Board), which was designed to check Medicare spending, based on the application of cost-benefit analysis. Despite denials by its creators, it’s a good bet that IPAB, or some other comparable entity, will morph into a rationing body for medical services. The rich and powerful will not be adversely affected by such bureaucratic edicts, but the rest of us will.
History has more than one way to ease us out of this world.
Next in the winter 2016 Issue
Unsafe Spaces
We Win, They Lose